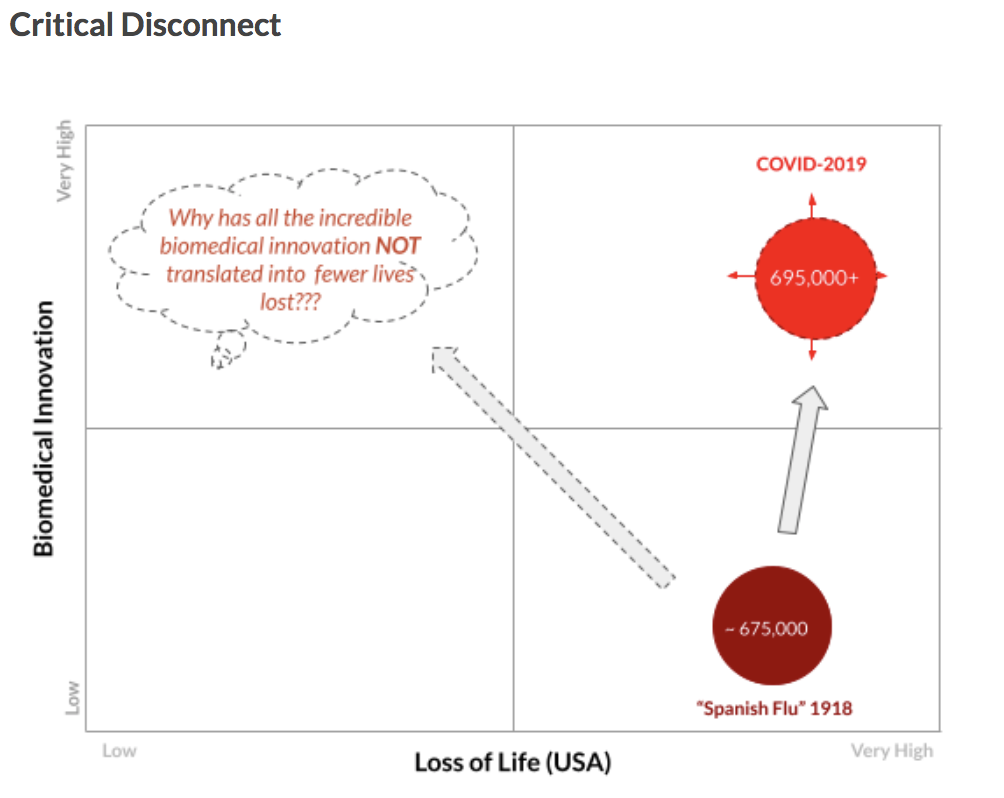
Novel biotechnologies and biomedical innovations are of great interest to me. Not just the science and technology but also the economics, policy, and ethical considerations. Over the past year, I have dedicated much of my blog posts to exploring novel innovations in biotechnology – the miracle of mRNA technology, COVID-19 vaccines, and the future mRNA marvels to come from such advancements. I have sought to answer critical questions such as: how we as a society have fared worse in the COVID-19 pandemic, despite the breakthroughs in technology, compared to the Spanish Influenza 100 years earlier. I explored challenges posed by the pandemic, often in real time, across ethical, business, legal and socio economic considerations. I warned early on about the chasm to go from vaccine development to vaccinations. I made a compelling case for global vaccine collaboration. I even estimated the economic business case for such global vaccine collaboration within a few million dollars of what was estimated by respected organizations such as the Rockefeller Foundation (Rockefeller Foundation).
My interest in biotechnology and biomedicine preceded the pandemic and will continue to extend well beyond. More broadly as I have been reading about the incredible advancements in biotechnology over the past four years, I have begun to develop a rather bold hypothesis:
I believe that we as a society stand at the dawn of a biotechnology renaissance. An upcoming period that has the potential, over the next decade or two, to more rapidly and meaningfully improve the health and well-being of humanity than in any other point in human history!
I will continue to elaborate on and evaluate this hypothesis in future blogs. Most importantly, whether or not we realize the full potential of these incredibly promising advancements in biotechnology will depend on whether we as a society are prepared to ethically and equitably manage these potentially life-changing biomedical innovations for the good of society at large.
As one example, recently I was struck by the positive early results to use cell therapy, not just to treat but to potentially cure type 1 Diabetes. Vertex Pharmaceuticals, a biopharmaceutical company, made headlines when its novel stem-cell therapy reversed Type 1 Diabetes in a single patient. Type 1 Diabetes has traditionally been a chronic disease in which the body cannot produce enough insulin. While the exact cause of the disease isn’t fully known, Type 1 Diabetes is considered to be caused by an autoimmune reaction – where the body’s immune system attacks the insulin-making beta cells of the pancreas (CDC). Often, people with Type 1 Diabetes are genetically predisposed. Epigenetics and outside life influences, such as a viral infection, can increase the likelihood of the disease. Once the gene is activated, the disease progresses. However, thanks to the research done by Vertex, a cure might finally be feasible.
In their first patient, a man who’d been suffering from Type 1 Diabetes for decades, Vertex’s therapy saw a resulting 91% daily drop in the required insulin doses previously necessary. They deemed it a potential “functional cure” – not necessarily a one-time cure, but one that allows the disease to be managed without consistent medication. The therapy is conducted through a series of synthetic islet cell transplants (Vertex). Islets are clusters of various cells – including beta cells – within the pancreas that help secrete Insulin. In Type 1 Diabetes, these cells are unable to naturally create the hormone. In traditional Islet transplants, Islets are isolated from 2 donors using various enzymes by a radiologist, who is able to guide these cells into the pancreas of the recipient. The goal is that these transferred cells achieve insulin independence and are able to create insulin on their own. Often, these transfusions are unsuccessful as the host body rejects the foreign Islet cells.
To solve this challenge, Vertex’s cure has Islet cells that are synthetically manufactured with novel immunoprotective devices. These devices are designed to evade recognition from the body’s immune system. This allows the cells to successfully transfer into the patient’s body. Transplantations are conducted via an injection, with an infusion of these synthetic insulin-producing cells” (clinicaltrials arena). Within 90 days post transfusion, the test patient was able to once again produce and maintain their insulin levels, effectively “curing” this disease. The potential of a stem-cell therapy as a cure for diabetes has the potential to be life-changing for millions of Type 1 Diabetes patients.
These advancements are incredibly exciting. Even curing one patient of Type 1 Diabetes is a huge accomplishment, one that I cannot wait to see replicated in future clinical trials. I will be eagerly following this novel biotechnology, its clinical trial outcomes, and broader application.
Beyond the exciting science, thinking about this advancement through my other PBH lenses raises some important questions. While this new cell therapy is still under development, I read that another breakthrough therapy from the same company for Cystic Fibrosis is priced at approximately $300,000 per patient per year (Fiercepharma). While Cystic Fibrosis is a rare disease affecting approximately 30,000 patients in the US, a chronic disease such as Type 1 Diabetes affects over 1.8 million people in the US, and millions globally. So, as I eagerly follow the incredible science and technology behind this promising new therapy, I will also be thinking about other important questions in my subsequent readings, research, and blogs:
- How can novel biotechnologies like gene and cell therapies be made more affordable, especially as they help cure not just rare diseases but more common, chronic diseases?
- How will patients and healthcare systems afford all these incredibly promising new therapies?
- How can we – society at large – make sure that these incredible biotechnology advancements help reduce, and not increase, healthcare inequalities in our society?